
English
version |
|||
|
Estos resúmenes son informes preliminares de proyectos en curso o de manuscritos en preparación. Enlace a WCN2007
|
Poster 1 - Poster 2 - Poster 3 - Poster 4
Epidemiology of renal disease
in a Hispanic population from Colombia: a review of regional renal biopsy
database
Luis F. Arias (1,3), Ariel Arteta (1,3), Alvaro García (2),
Gonzalo Mejía (2), Jorge Henao (2), Inge H. Arroyave (2), Nelson
Carvajal (2), Jorge L. Arango (2), Alberto Reino (2), Joaquin A. Rodelo
(2), Rubén D. Giraldo (1,3), Mónica Gil (1), Fernando Bolaños
(1), Mario Arbeláez (2).
Departments of (1)Pathology and (2)Nephrology, and (3)PRYT Group, Faculty
of Medicine, University of Antioquia, Medellín, Colombia. luisfer_uda@yahoo.com
Epidemiological data of biopsied renal disease provide useful information in clinical practice and investigation. Large renal biopsy registries are available and recent works have demonstrated changing frequencies of glomerulopathies. FSGS is more frequent in African-Americans, and some works have shown a high incidence in Latin-American people. This study was aimed at determining the pattern of renal diseases diagnosed by biopsy in a region of Colombia and it represents the basis for future works in Hispanics, and is intended to serve as a source of information for nephrologists concerned with Latin America renal pathology.
Methodology. This is a single-centre-based retrospective analysis. All native renal biopsies of our archives, from 08/1998 to 10/2006, were revised and histologic slides revaluated for two pathologists. We exclude biopsies of patients with urinary tract disease, malformations, trauma, or neoplasm as unique cause of the renal disease.
Results. The total number of native kidney biopsies was 1092; 92 cases were excluded: 74 due to unsatisfactory sample; 11: normal renal tissue; and 7: a diagnosis can not be done; then, the number of cases was 1,000. Mean patient age was 29.7±18.1 years-old (range: 1-78); 46.5% were males. Primary glomerulonephritis (GN) occurred in 79.4%; lupus nephritis in 11.4%; tubulointerstitial diseases in 3.7%; vascular diseases in 2.8%; and other secondary diseases in 2.7%. In patients with glomerulopathies (excluding lupus nephritis) (n = 794), the more frequent histologic diagnosis was FSGS (31.2%), followed by IgA nephropathy (IgAN) (23.7%), membranous GN (9.7%), minimal change disease (8.6%), diffuse endocapillary GN (7.8%), postinfectious GN (6.7%), diffuse crescentic GN (5.3%), membranoproliferative type I GN (3.7%), non-IgA mesangial proliferative GN (1.4%), and others (2.0%).

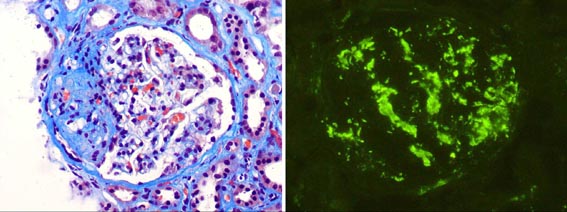
Figure 2. The most frequent glomerulopathy in our Hispanic patients is focal and segmental glomerulosclerosis, followed by IgA nephropathy. Left: a FSGS case, Masson’s trichrome, x400; right: Mesangial IgA deposits in a IgAN case, IF for IgA, x400.
Conclusions. FSGS was the most common pattern of primary GN and IgAN the second, highlighting similarities with other western countries. The same that African-Americans, in our group (Hispanics) FSGS is the more frequent glomerulopathy, but differently to those, in these IgAN is very frequent. The reasons for this behaviour are unclear and warrant further investigations; it could be due to genetic and/or environmental factors. The information obtained from these results is an important contribution for the understanding of the prevalence in renal diseases in Latin America.
Bibliography
- Nair R, Walker PD. Kidney Int 69:1455-8, 2006
- Covic A, Schiller A, Volovat C, et al. Nephrol Dial Transplant 21:419-24,
2006
- Bahiense-Oliveira M, Saldanha LB, Mota EL, et al. Clin Nephrol 61:90-7,
2004
- Korbet SM, Genchi RM, Borok RZ, Schwartz MM. Am J Kidney Dis 27:647-51,
1996
Glomerular tip lesion: Clinical
outcome and comparison to focal segmental glomerulosclerosis in Hispanic
patients
Luis F. Arias (1,3), Ariel Arteta (1,3), Alvaro García (2),
Gonzalo Mejía (2), Jorge Henao (2), Nelson Carvajal (2), Jorge
L. Arango (2), Alberto Reino (2), Joaquin A. Rodelo (2), Rubén
D. Giraldo (1,3), Mónica Gil (1), Fernando Bolaños (1),
Mario Arbeláez (2).
Departments of (1)Pathology and (2)Nephrology, and (3)PRYT Group, Faculty
of Medicine, University of Antioquia, Medellín, Colombia. luisfer_uda@yahoo.com
The clinical significance of the glomerular tip lesion (GTL), defined by the presence of at least 1 segmental lesion involving the tip domain with either adhesion between the tuft and Bowman’s capsule, or confluence of podocytes with parietal or tubular epithelial cells, at the tubular lumen or neck, without perihiliar or collapsing lesions, remains unclear. It is controversial the relation of GLT to minimal change disease (MCD) and focal segmental glomerulosclerosis (FSGS). With the aim to determine the clinical and histological features, and natural history of GTL, we retrospectively review our cases of Hispanic patients with this glomerular lesion.
Methodology. This is a single-centre-based retrospective analysis. All native renal biopsies diagnosed as FSGS between 08/1998 and 10/2006 were revised for cases with GTL. Glomerulosclerosis (GS), percentage of glomeruli with segmental lesions, and interstitial fibrosis (IF) were quantified. All biopsies come from Hispanic patients. Clinical information and follow-up data were registered for analyses.
Results. Between 248 cases diagnosed as FSGS, 37 correspond to GTL (14.9%). Mean age was 22.1±17.1 years (range 1-65); 19 (51.4%) patients were children, and 56.8% were males. At presentation 36 cases (97.3%) had nephrotic syndrome (NS): mean proteinuria 5.9 ± 4.1 g/24h. Glomerular lesions included GTL alone in 25 cases (67.6%), and GTL with peripheral and/or indeterminate lesions in 12 (32.4%). There were not significant differences for age, serum creatinine (Cr), creatinine clearance (CrCl), and proteinuria level between cases with no other specification (NOS) variant of FSGS and GTL. IF, GS, and percentage of glomeruli with segmental lesions were higher in NOS than GTL: 13.4%, 11.8%, and 29.8% versus 4.9%, 3.2%, and 18.3% respectively (P<0,01). Follow-up data were available in 24 patients, of whom 15 received steroids alone and 9 steroids and a cytotoxic agent. At a mean follow-up of 20.5±19.1 months (range 3.0 to 60.8) 7 patients (29.2%) achieved chronic kidney disease, 11 (45.8%) had persistent nephrotic proteinuria or partial remission, and 6 (25%) achieved complete remission.
Table 1. Comparison between NOS and GTL variants of FSGS
| Characteristics | FSGS NOS | GTL | P |
| n | 196 | 37 | |
| Age (years) | 25.8 ± 18.0 | 22.1 ± 17.1 | 0.28 |
| Global GS | 16.3 ± 22.0 | 3.2 ± 7.4 | 0.001 |
| % glomeruli with segmental lesions | 33.8 ± 27.7 | 18.3 ± 15.0 | 0.002 |
| Total glomeruli with lesions | 41.5 ± 30.1 | 20.3 ± 17.2 | <0.001 |
| % interstitial fibrosis | 16.6 ± 14.3 | 4.9 ± 7.7 | <0.001 |
| Arteriolar hyalinosis | 64 (33%) | 4 (11%) | 0.009 |
| Hypertension | 102 (52%) | 14 (38%) | 0.151 |
| Proteinuria at presentation (g/d) | 5.5 ± 6.4 | 5.6 ± 4.4 | 0.931 |
| Higher proteinuria (g/d). a | 7.3 ± 7.9 | 9.2 ± 6.3 | 0.275 |
| SCr at presentation (mg/dL) | 1.2 ± 1.2 | 1.5 ± 1.9 | 0.541 |
| CrCl at presentation (mL/min) | 81.1 ± 36.6 | 88.3 ± 32.8 | 0.415 |
| CKD b | 30 (34%) | 7 (29%) | 0.807 |
| No or partial remission b | 49 (86%) c | 11 (64%) c | 0.075 |
| Complete remission b | 8 (14%) c | 6 (35%) c | 0.075 |
| Outcome (Remission Vs. No or partial Vs. CKD) b | 9% - 56% - 35% | 25% - 46% - 29% | 0.156 |
FSGS NOS: focal segmental glomerulosclerosis no otherwise
specification; GTL: glomerular tip lesion; GS: glomerulosclerosis; SCr:
serum creatinine; CrCl: creatinine clearance; CKD: chronic kidney disease.
a: At any follow-up time.
b: Follow-up in 87 NOS cases and 24 GTL cases
c: Percentage of cases without chronic kidney disease.
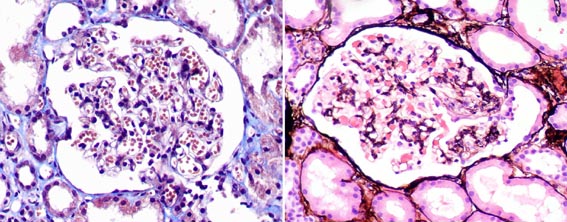
Figure 1. Glomeruli with characteristic tip lesions. It can be adhesion of the tuft to Bowman’s capsule at the tubular neck or confluence of podocytes with parietal or tubular cells at the tubular lumen or neck, as seen in both images. Tuft peripheral lesions, without a clear relation with tubular origin, are called “indeterminate”, and they can not be defining of GTL. (Left: Masson’s trichrome, right: H&E; x400).
Conclusions. GTL is a distinctive morphological glomerular alteration related to NS, with many similarities to NOS variant FSGS and that may have an aggressive course, although GLT show less chronic renal changes. In our series of Hispanic patients we do not have a “favourable prognosis” and this entity was similar to FSGS in its clinical outcome.
Bibliography
- Howie AJ, Pankhurst T, Sarioglu S, et al. Kidney Int 67:987-1001, 2005
- Stokes MB, Markowitz GS, Lin J, et al. Kidney Int 65:1690-702, 2004
Primary focal segmental glomerulosclerosis
histological variants in Hispanic children and adolescents with nephrotic
syndrome
Andrea Múnera (1), Natalia Ortiz (1), Rubén D. Giraldo
(1,4), Ariel Arteta (1,4), Liliana Rubio (2), Claudia Prada (2), Alvaro
García (3), Gonzalo Mejía (3), Jorge Henao (3), Fernando
Bolaños (1), Mónica Gil (1), Joaquin A. Rodello (2), Alberto
Reino (2), Luis F. Arias (1,4).
Departments of (1)Pathology, (2)Pediatric Nephrology, (3)Nephrology, and
(4)PRYT Group, Faculty of Medicine, University of Antioquia, Medellín,
Colombia. luisfer_uda@yahoo.com
Focal segmental glomerulosclerosis (FSGS) is not a single disease, but a lesion that includes several distinct glomerular changes. A recent working classification system has distinguished five FSGS variants that may have prognostic value. We evaluated our cases of Hispanic children and adolescents with FSGS and determine histologic variants, clinicopathological presentation, and outcome.
Methodology. Between 342 native kidney biopsies (1,988 – 2,006) from patients aged 18 or less, 68 (19.9%) have the confirmed diagnosis of FSGS and were included in this work. All biopsies come from Hispanic patients and they had nephrotic syndrome. Biopsies were classified by histologic variants. Clinical information and follow-up data were registered.
Results. Forty-two
cases (61.8%) were males; mean age: 9.9±5.9 years (0-18). FSGS
was classified as no other specification (NOS) variant in 43 cases (63.2%),
tip lesion (GTL) in 19 (27.9%), collapsing (COLL) in 5 (7.4%), and cellular
(CELL) in 1 (1.5%); there was no cases of perihiliar variant. Twelve cases
(17.6%) developed chronic kidney disease (CKD). Mean follow-up was 772±1,005
days (90-4,745). There is not association between histologic variant and
serum creatinine (Cr) at diagnosis, creatinine clearance (CrCl) or CKD.
Proteinuria at diagnosis is significantly higher in patients with COLL
(P<0.01). There is more global glomerulosclerosis percentage (GS):
10.6%, and more interstitial fibrosis (IF): 12.3% in patients with NOS
than GTL: 0.4% and 2.4% respectively (P<0.01). COLL shows intermediate
values for GS and IF. CrCl at diagnosis is correlated to GS, IF, and hyaline
arteriolosclerosis (ha) (P<0.01); GS, IF, and ha do not show association
with proteinuria. Percentage of glomeruli with segmental lesions is correlated
to proteinuria (P=0.02), but does not with renal function. Hypertension
was associated with GS (P=0.04), percentage of glomeruli with segmental
lesion (P=0.01), and Cr at diagnosis (P=0.03).
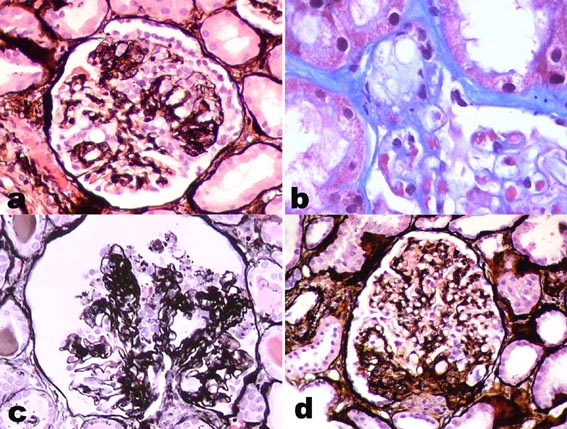
Figure 1. In this microphotography we can see the four more frequent variants of FSGS. a. NOS variant. b. Tip lesion. c. Collapsing lesion. d. Perihiliar variant. (a, c, and d: methenamine-silver, x400; b: Masson’s trichrome, x600).
Conclusions. Histological characteristics observed in our Hispanic patients apparently are comparable with other published series. NOS and COLL variants of FSGS show more chronic renal changes at diagnosis than GTL. COLL variant is associated with more severe proteinuria. Variants do not show association with CKD (at least in this short follow-up). Histologic chronic changes are associated with renal function, and glomerular segmental lesion with proteinuria severity.
Bibliography
- Abrantes MM, Cardoso LS, Lima EM, et al. Pediatr Nephrol. 21:482-9,
2006
- Thomas DB, Franceschini N, Hogan SL, et al. Kidney Int 69:920-6, 2006
- Srivastava T, Simon SD, Alon US. Pediatr Nephrol 13:13-8, 1999
BK virus infection in renal allografts
in colombia: experience of the one center
Alberto C. Reino (a), Luis F. Arias (b), Joaquin R.. Rodelo (a), Gonzalo
Mejia (a), Ariel Arteta (b), Jorge E. Rico (a), Maria X. Cardona (a),
Jose N. Carvajal (a), Alvaro Garcia (a), Jorge L. Arango (a) Jorge E.
Henao (a), and Mario Arbelaez (a).
(a)Section of Nephrology and (b)Department of Pathology, Faculty of Medicine,
University of Antioquia, Medellín, Colombia. sarracana@yahoo.com
BK Virus (BKV) infection is a growing problem in kidney transplantation (KT). Interstitial nephritis is the most important pathology caused by the virus leading to graft failure and the need for dialysis treatment. Reactivation of the virus has been documented in conditions associated with impaired immunity, such as, organ transplantation. We show our experience with 10 patients who had histologically documented BKV nephropathy (BKVN) from July 1998 to June 2006.
Methodology. We revised retrospectively 713 renal allograft biopsies from 464 patients underwent KT between July 1998 and June 2006. These biopsies were evaluated by light microscopy searching for viral inclusions characteristics of the infection. For confirmation of the infection, polymerase chain reaction (PCR) assay for BKV DNA was performed in three cases. Negativity for CMV was demonstrated by immunohistochemistry. Ten patients were identified since 1998.
Results. Ten
cases (1.4%) among 713 renal allograft biopsies was identified (2.2% among
464 biopsied patients). Five were males. Mean age: 39.1±16.4 years
(14-70). All patients received deceased donor kidney transplant. Mean
HLA mismatch: 4.4±1.1. Immunosuppression: prednisone, CyA (8) or
Tac (2), and MMF (8) or azathioprine (2). No one received anti T cell
antibodies, but one received anti-CD25 (Daclizumab). All patients had
renal dysfunction, mean serum creatinine (sCr): 3.8±1.7 (2.3-7.8).
Mean time between KT and renal biopsy: 7.3±4.7 months (3.4–19.5).
Eight out of 10 patients had at least one acute rejection episode prior
to BKV diagnosis. All had interstitial nephritis; plasm cell are very
frequent; in some cases tubulitis is found; inclusions are exclusively
nuclear, with chromatin margination, these are basophilic or granular
clear; percentage of tubular cells with inclusions is approximately 3%
to 15%.
Mean post-KT follow-up: 24.3±25 months. Five patients lost the
graft, mean time lost graft after diagnosis: 95.6±68.6 days (12–203).
Mean lattest sCr: 4.5±2.4 mg% (1.3–8.6) (P: 0.02 compared
to sCr at diagnosis).
Diagnosis in 6 cases was done retrospectively (cases before 2004), 4 who
lost their graft, in 2 the immunosuppression was reduced due to suspected
CMV disease and sCr improved. The other four cases were diagnosed at time
of renal biopsy; immunosuppression was reduced in these 4: 1 improved,
1 remains stable, 1 lost the graft, and another died by sepsis. None received
antiviral therapy for BKV.

Figure 1. Inclusions are evidenced in the images a and b; these are exclusively intranuclear and infected tubules show cellular desquamation and are surrounded by inflammatory cells (H&E, X400). In images c and d we can see “decoy cells” with the typical intranuclear inclusions, degenerative cytoplasmic changes and aspect in “comet cell”; this changes are very characteristic for BKV replication (Papanicolau stain, x400).
Conclusions. Incidence of BKV-associated interstitial nephritis is variable in different centers. Ours results does not show differences on clinical presentation with other non Latin-American centers. In many of our cases steroid bolus preceded the BK detection, however it is possible that dysfunction that cause bolus treatment do not be due to rejection but BK associated interstitial nephritis. BKVN is a great problems among kidney transplant recipient, due to carry a bad prognosis with high rate lost graft.
Bibliography
- Barri YM, et al. Clin Transplant 2001; 15(4):240-246.
- Ramos E, et al. J Am Soc Nephrol 2002; 13:2145-2151.
- Brennan DC, et al. Am J Transplant 2005; 5:582-594.